Stefano Ricci
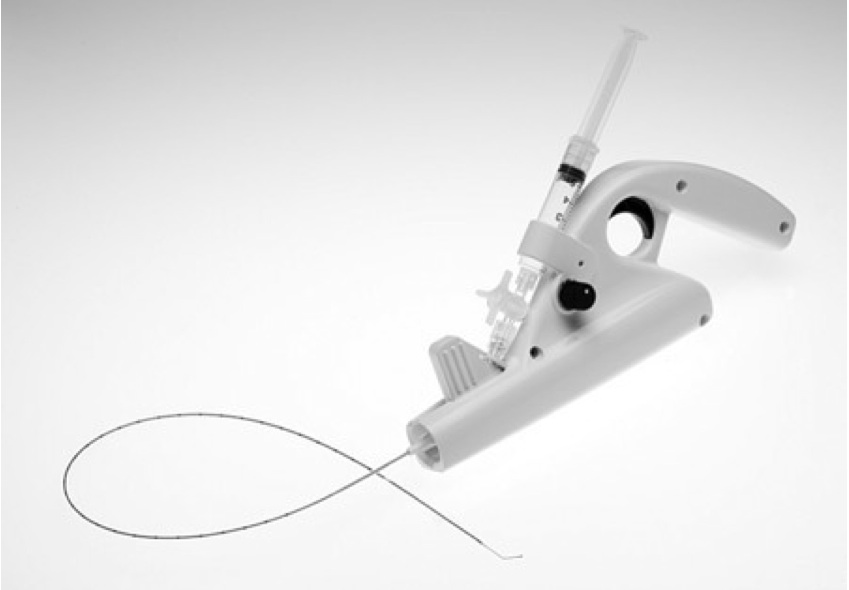
AbstractA new mechanochemical device, (ClariVeinw, Madison, CT, USA), that does not require a generator or the use of tumescent anesthesia, was developed to achieve venous occlusion utilizing a wire rotating within the lumen of the vein at 3500 rpm that abrades the intima to allow for improve the efficacy of the sclerosant. A liquid sclerosant (sodium tetradecyl sulphate) is concomitantly infused through an opening close to the distal end of the catheter near the rotating wire. The wire tip is positioned 2 cm from the saphenofemoral junction under ultrasound guidance. With the wire rotating and during sclerosant infusion, the catheter is pulled down the vein at a rate of approximately 1–2 mm per second. Catheter wire rotation is first activated for 2–3 s at the highest speed setting to create venospasm which minimizes forward flow into the common femoral vein. This is a single-use device that can be inserted through a 4 or 5 French guiding catheter with local insertion site anesthesia only, without the need for tumescence anesthesia. The system includes an infusion catheter, motor drive, stopcock and syringe. |
|
ClariVeinw |
Some questions have been raised by this interesting report:
What is the destiny of the largely mobilized endothelium into the venous stream?
When two modalities are combined, how can you say that the final result is due to the combination of the two or only to one of the methods? Have you carried out a trial with abrasion alone, for example?
Why did you choose to use liquid sclerosant instead of foam (which has a better performance, but also better visualization on US)?
Did you ever observe any adverse events during initial device development? Did you use animal models? Could you study histological GSV evolution?
What will be the average cost of the device, compared to the low costs of foam sclerotherapy?
What is the appearance of the closed vein at 260 days? Is there any difference between this and a foam-sclerosed vein?
These questions were put to the Author but we have not yet received a reply.
[TOP]