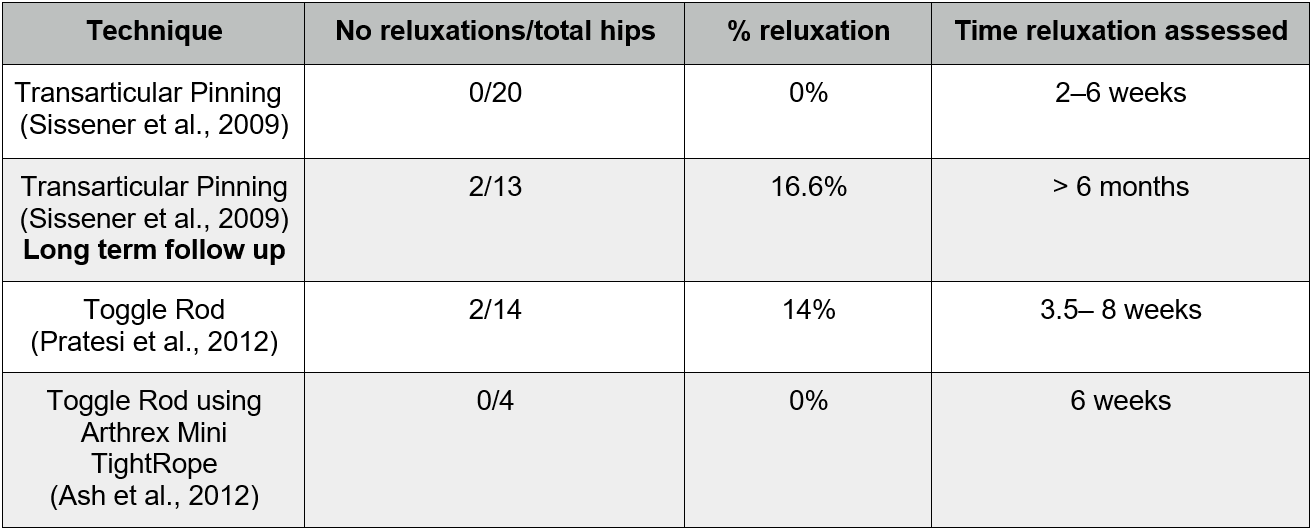
Table 1: Reluxation rates and assessment times for the 3 studies
Reluxation Rates Following Different Techniques for Open Stabilisation of Feline Coxofemoral Dislocations
a Knowledge Summary by
Elly Russell MA, VetMB, Cert AVP, MRCVS 1*
1The Minster Veterinary Ptactice, Salisbury Road, York, YO26 4YN
*Corresponding Author (ellythevet@hotmail.com)
Vol 4, Issue 1 (2019)
Published: 24 Jan 2019
Reviewed by: Andy Morris (BSc(Hons) BVSc CertAVP(GSAS) MRCVS) and Stephen Jones (MVB, MS, DACVS)
Next review date: 24 Jan 2021
DOI: 10.18849/VE.V4I1.185
In cats with craniodorsal coxofemoral luxation does surgical stabilisation using a toggle rod technique result in a lower rate of reluxation than using a transarticular pin?
Clinical bottom lineThere is currently insufficient evidence to identify if transarticular pinning or a toggle rod technique result in lower rates of reluxation following surgical management of craniodorsal coxofemoral luxations in cats.
Both transarticular pinning and toggling using the Arthrex Mini TightRope system with Arthrex FiberWire suture resulted in 0% reluxation rates at short-term radiographic follow up with 0/20 joints reluxated at 2–6 weeks post-transarticular pinning and 0/4 joints reluxated at 6 weeks post-toggling.
Toggling using an IMEX toggle (IMEX Veterinary Inc.) and polydioxanone (PDS II, Ethicon) suture had a higher reluxation rate of 14% (2/14 joints) at 3.5 to 6 weeks postsurgery.
Longer term follow up of joints stabilised using transarticular pinning found 16.6% reluxation (2/13 joints) when radiographed at least 6 months after surgery.
Small sample sizes, and variations in the length of follow up, inclusion and exclusion criteria and surgical technique significantly challenges any conclusions that may be drawn.
It does appear that reluxation rates for all three techniques investigated here compare favourably to generally quoted reluxation rates following open reduction (28% quoted by Rochereau et al., 2012) and that the use of all reported techniques can be justified for the management of craniodorsal coxofemoral luxations in cats.
Clinical scenario
A 4 kg 3-year-old male neutered domestic short-haired cat has been presented to you following a road traffic accident. After initial stabilisation, radiographs have identified a craniodorsal luxation of the right coxofemoral joint. Closed reduction was performed but the joint could not be maintained in reduction. No concurrent orthopaedic or other body system injuries have been identified. You advise the owners that surgical stabilisation would be the best course of action, particularly for a young active cat, and whilst the patient is not insured the owners are happy to make funds available for surgery at your practice. You have previously performed stabilisation of coxofemoral luxations in three feline patients using the transarticular pinning technique and whilst two patients recovered uneventfully, the third experienced reluxation. A colleague has recently attended a CPD course on treatment of common feline orthopaedic conditions and advises you that stabilisation using a toggle rod technique results in lower reluxation rates. You wonder which procedure should be performed in this case.
The evidence
Three studies were identified which addressed the PICO question and fitted the inclusion and exclusion criteria applied. All the studies identified were noncomparative case series. The number of cases included in the studies was low: 4, 14 and 20 (median 14). Some other case series reporting outcomes for both feline and canine patients were excluded due to the low number of feline patients (three or less), along with a number of case reports.
All three studies described a surgical technique used for the open reduction and stabilisation of craniodorsal coxofemoral luxations in feline patients from a referral population. Two of the studies (Sissener et al., (2009) and Pratesi et al., (2012)) presented only feline patients, whilst Ash et al., (2012) presented findings for four feline patients and five small dogs. Only the results as they applied to the feline patients were considered.
Sissener et al., (2009) described the use of transarticular pins (1.6 mm diameter in the majority of cases with 1.2 mm and 2.0 mm pins also used) left in-situ for between 2 to 6 weeks in 20 cases. Radiographic follow up was performed at pin removal and, for 12 of the cases, at a time point > 6 months postsurgery. No reluxations were identified at short-term follow up, but two patients radiographed > 6 months later demonstrated reluxation. In addition to reluxation, complications included a bent 1.2 mm pin identified 6 weeks postoperatively in one patient and spontaneous resorption of the femoral head and neck identified 6 months postoperatively in another.
Pratesi et al., (2012) described a toggle rod technique used in 14 cases. A 3.2 mm IMEX toggle rod with two strands of 4 metric polydioxanone was used for the majority of cases. In two cases three strands of 4 metric polydioxanone were used and in one case the polydioxanone size was increased to 5 metric. A single case also had a smaller 2.7 mm toggle used. Short-term radiographic follow up was performed at 3.5–8 weeks postoperatively, revealing two patients had suffered reluxations. No other complications were reported.
Ash et al., (2012) applied an identical technique to all four feline cases, using an Arthrex Mini TightRope toggle and Arthrex FiberWire suture. No reluxation was noted at 6 week postoperative radiographs and none of the feline patients experienced any other complications.
Reluxation rates including time of assessment for all three studies are summarised in the following table (Table 1):
All three studies also presented other, subjective, outcome measures that were not directly applicable to the PICO question. These included lameness assessments performed by a veterinarian and owner outcome questionnaires conducted by telephone. Along with the subjective nature of these assessments, all studies failed to describe observer standardisation, introducing observer bias, and time to follow up with owners varied widely introducing recall bias.
Summary of the evidence
| Population: | Feline patients presenting to two referral centres with craniodorsal coxofemoral luxation and selected for surgical management using transarticular pinning between 1998 and 2003.
Selection criteria for use of this technique were:
This resulted in 17/20 patients with concurrent orthopaedic injuries, two patients where closed reduction and Ehmer sling application had failed and a final patient with no previous reduction attempts or concurrent injuries. Patients ranged from 6 months to 12 years. |
| Sample size: | 20 cats (21 coxofemoral joints) n = 20 |
| Intervention details: |
|
| Study design: | Retrospective dual-centre case series |
| Outcome Studied: |
|
| Main Findings (relevant to PICO question): |
|
| Limitations: |
|
| Population: | Feline and small canine patients presenting to a single referral centre for management of traumatic craniodorsal coxofemoral luxation and undergoing surgical stabilisation using a toggle technique (Arthrex TightRope and Mini TightRope systems). For feline patients, trauma to surgery ranged from 2–4 days, and patients’s weights ranged from 3.7–4.7 kg. All were domestic short-haired cats. Presence of any concurrent injuries is not given. Patients were excluded if there was radiographic evidence of periarticular fractures, hip dysplasia or osteoarthritis. |
| Sample size: | 4 felines and 5 canines n = 4 relevant to PICO |
| Intervention details: |
|
| Study design: | Retrospective single centre case series |
| Outcome Studied: |
|
| Main Findings (relevant to PICO question): |
|
| Limitations: |
|
| Population: | Feline patients presenting to single referral centre for management of unilateral craniodorsal coxofemoral luxation. Cases represent consecutive cases managed by toggle rod stabilisation. Mean days from trauma to surgery was 3.2 days (range from 1–6 days). 9/14 patients are reported to have concurrent orthopaedic injuries and 3/5 patients presenting with coxofemoral luxation only had small articular bone fragments from either femoral head or dorsal acetabular rim. In six cases a referring vet had attempted closed reduction. Patients’s weight ranged from 2.8–6.8 kg, ages from 7 months to 10 years and breeds were 11 domestic short-haired, 1 domestic long-haired and 2 British short-haired cats. |
| Sample size: | 14 cats n = 14 |
| Intervention details: |
|
| Study design: | Retrospective single centre case series |
| Outcome Studied: |
|
| Main Findings (relevant to PICO question): |
|
| Limitations: |
|
Appraisal, application and reflection
There is a lack of high quality evidence available to address the clinical question as all of the relevant studies identified and appraised here are retrospective case series. These sit low on the hierarchy of evidence and, particularly as they are not comparative studies, are not appropriate for assessing the impact of a specific surgical technique on outcome. Randomised, controlled, blinded studies that compare the two surgical techniques are needed to generate high quality evidence on which to base clinical decisions.
A large number of surgical stabilisation procedures are described for the management of coxofemoral luxation, but there is little evidence to guide technique choice (Moore, 2006). Reluxation is reported to be the most common complication following open reduction and surgical stabilisation of coxofemoral luxations. Rochereau et al., (2012) reports rates of around 28% for a variety of open reduction techniques including extra-articular stabilisation and ventral approach for the placement of stainless steel rope cases. It should be noted that many of the studies quoted examine reluxation rates for studies in dogs only. The reluxation rates quoted in all the studies (Table 1) appear to compare favourably with this, providing some evidence to support the use of these techniques. However, alongside the low case numbers, the variability in follow up time reduces the quality of information generated. In addition to this, none of the three studies described standardise the observer for short-term follow up radiographic assessments and whilst presence of coxofemoral luxation on a radiograph is relatively objective, observer bias is possible.
Longer-term radiographic follow up is only performed in the transarticular pinning study (Sissener et al., 2009). It is interesting that reluxation was first identified at least 6 months after surgery, at least 5 months after pin removal, in two cases. Ash et al., (2012) argues that 6 week follow up is adequate for assessing reluxation rates since long term periarticular fibrosis is responsible for stability after this stage and reluxation rates beyond this time frame are very low. However, the findings of the Sissener et al., (2009) study suggest that longer-term follow up is important in establishing reluxation rates. The evidence generated by these studies would be more valuable if follow up was standardised and long term, greater than 12 months, follow up was available for all the surgical techniques.
All of the studies identified describe management of cases at referral centres. This means the cases reported are unlikely to directly reflect those managed in the primary care setting. Specifically, cases are likely to have a higher incidence of concurrent injuries and for more time to have elapsed between luxation and treatment. Both of these factors might be expected to increase reluxation rates. Pre-surgical management is also variable and variably reported. Duration of luxation is not reported by Sissener et al., (2009) whilst pre-referral management is not described by Ash et al., (2012). Postoperative care is also affected by management of concurrent injuries and therefore the patients in these studies are not always subject to the same postoperative management, which would be expected to impact on reluxation rates.
Differences in inclusion and exclusion critera, or the lack of these criteria, across the studies compromises the ability to compare reluxation rates for the different surgical procedures. Ash et al., (2012) excludes patients with radiographic evidence of periarticular fracture, hip dysplasia or osteoarthritis whilst Pratesi et al., (2012) includes two patients with suspected pre-existing hip dysplasia (HD) and three with periarticular bone fragments. Sissener et al., (2009) details inclusion criteria including concurrent injuries and failure of previous surgical stabilisation but does not mention HD or periarticular fractures. It is interesting to note that one of the 2/14 cases experiencing reluxation in the Pratesi et al., (2012) study had hip dysplasia since pre-existing pathology such as this might be expected to impact upon the success of open reduction and stabilisation of traumatic luxations. For this reason, inclusion of these cases in the Pratesi et al., (2012) and possibly in the Sissener et al., (2009) study limits the conclusions we can draw on reluxation rates from these studies.
For the transarticular pinning technique, accurate placement of the transarticular pin is crucial for correct seating of the femoral head in the acetabulum, which is very likely to correlate with reluxation rates. Sissener et al., (2009) reports three separate methods for pin placement were used, it would be useful to assess if any of these methods resulted in a better outcome. Similarly, pin size selection is poorly described and weight, which we would expect to guide size selection, is omitted from signalment. Evidence to guide pin size selection and placement technique would be useful but is lacking.
For the toggle techniques, Pratesi et al., (2012) uses different toggle sizes, suture sizes and thread numbers. Reasons for these variations are not always stated (although one patient received three strands of suture due to suspected pre-existing HD) and there is no obvious trend, for example increasing suture size or number with increasing patient weight. Again, the variation in surgical technique limits the conclusions we are able to draw about reluxation rates, and the study fails to generate guidelines for selection of toggle size or suture.
The surgical technique described by Ash et al., (2012) is consistently applied across all cases, which allows better assessment of the procedure’s impact on reluxation rates. The toggle system reported by Pratesi et al., (2012) used both different toggle (Arthrex Mini- TightRope) and suture (Arthrex FiberWire) than the Ash et al., (2012) study. Suture type/strength and toggle construct are likely to impact upon reluxation rates. This limits the potential to combine data about ‘toggle procedures’ from these two studies (Ash et al., 2012 and Pratesi et al., 2012). Further, this difference in suture material highlights again the need for longer-term follow up, since polydioxanone utilised in the Pratesi et al., (2012) study will lose tensile strength at around 3–4 weeks, whilst the Arthrex FiberWire is more durable. The discovery of reluxation > 6 months postoperatively (Sissener et al., 2009) might suggest that maintaining reduction requires more persistent implants and that periarticular fibrosis alone may be insufficient.
It should be noted that Sissener et al., (2009) reports owner outcomes for the patients with reluxations > 6 months postoperatively to be very good and Pratesi et al., (2012) describes limb use as good despite reluxation within 6 weeks of surgery in two cases, one of which received no further treatment. It is important to consider if reluxation is the most clinically useful outcome measure. All the studies include other outcome measures, all subjective, including veterinary lameness assessments without observer standardisation and owner questionnaires completed at very wide ranging time points. Long-term degenerative joint disease may be a more important clinical comparator between surgical techniques and more objective outcome measures such as measuring ground reaction force on pressure sensitive walkways (Schnabl et al., 2015) could be considered.
In general, the studies fail to generate any descriptive rationale for the selection of one surgical procedure over another. All the cases in the Ash et al., (2012) study seem to have been managed using the toggle technique, and similarly in the Sissener et al., (2009) study for the pinning technique, whilst Pratesi et al., (2012) implies not all presenting cases were managed with the toggle technique but does not explain the choice of this technique for these cases.
Further studies using randomised, controlled, blinded trials comparing two standardised surgical techniques, ideally in a primary care setting, with objective outcome measures are needed.
Methodology Section
| Search Strategy | |
| Databases searched and dates covered: | CAB Abstracts on CABI direct platform 1973 to week 8 2018
MEDLINE on OVID platform 1946 to week 8 2018 Scopus 1973 to week 8 2018 Web of Science 1973 to week 8 2018 |
| Search terms: | (cat OR cats OR feline OR felines) AND (hip dislocation OR hip luxation OR coxofemoral dislocation OR coxofemoral luxation) AND (transartic* OR transtroch* OR pin* OR togg* OR rod) |
| Dates searches performed: | Feb 25th 2018 |
| Exclusion / Inclusion Criteria | |
| Exclusion: |
|
| Inclusion: | Correct species, craniodorsal luxation managed surgically with technique recognisable as transarticular pinning or toggle rod with outcome measures including reluxation. |
| Search Outcome | ||||||
|
Database |
Number of results |
Excluded – non-English language publication |
Excluded – Case reports, Reviews, Conference proceedings |
Excluded – Does not address PICO question |
Excluded – Full text not available |
Total relevant papers |
|
CAB Abstracts |
21 | 6 | 5 | 7 | 1 | 2 |
|
MEDLINE |
14 | 1 | 1 | 9 | 1 | 2 |
|
Scopus |
8 | 2 | 1 | 3 | 0 | 2 |
|
Web of Science |
38 | 7 | 3 | 25 | 0 | 3 |
|
Total relevant papers when duplicates removed |
3 | |||||
The author declares no conflict of interest.
Intellectual Property Rights
Authors of Knowledge Summaries submitted to RCVS Knowledge for publication will retain copyright in their work, and will be required to grant to RCVS Knowledge a non-exclusive licence of the rights of copyright in the materials including but not limited to the right to publish, re-publish, transmit, sell, distribute and otherwise use the materials in all languages and all media throughout the world, and to licence or permit others to do so.
Disclaimer
Knowledge Summaries are a peer-reviewed article type which aims to answer a clinical question based on the best available current evidence. It does not override the responsibility of the practitioner. Informed decisions should be made by considering such factors as individual clinical expertise and judgement along with patient’s circumstances and owners’ values. Knowledge Summaries are a resource to help inform and any opinions expressed within the Knowledge Summaries are the author's own and do not necessarily reflect the view of the RCVS Knowledge. Authors are responsible for the accuracy of the content. While the Editor and Publisher believe that all content herein are in accord with current recommendations and practice at the time of publication, they accept no legal responsibility for any errors or omissions, and make no warranty, express or implied, with respect to material contained within. For further information please refer to our Terms of Use.